Free DD 149 Template
The DD 149 form is an essential document for veterans seeking to request a correction of military records. This form plays a critical role in ensuring that service members can rectify any inaccuracies or discrepancies that may exist in their official military documents. It is often used to address issues related to discharge status, awards, and other important details that can affect a veteran's benefits and overall recognition. Completing the DD 149 requires careful attention to detail, as it necessitates providing personal information, a clear explanation of the requested changes, and any supporting documentation that may bolster the case. Veterans must also be aware of the specific procedures involved in submitting the form, including where to send it and any associated timelines. Understanding the significance of the DD 149 form can empower veterans to advocate for their rights and ensure that their military service is accurately reflected in their records.
Document Specifics
| Fact Name | Description |
|---|---|
| Purpose | The DD Form 149 is used to apply for a correction of military records. |
| Eligibility | Any former or current service member can submit this form to request changes. |
| Submission Process | Applicants must complete the form and send it to the appropriate board for review. |
| Supporting Documents | Additional documentation may be required to support the correction request. |
| Governing Law | The process is governed by Title 10, United States Code, Section 1552. |
| Decision Timeline | Decisions are typically made within six months, but it can vary based on the case. |
Similar forms
- DD Form 214: This document serves as a certificate of release or discharge from active duty. Like the DD 149, it provides essential details about a service member's military history and is crucial for veterans seeking benefits.
- New York MV51 form: This certification document is crucial for the sale or transfer of vehicles from 1972 or older, requiring proper documentation for private sales. It can be accompanied by supporting documents, such as bills of sale, available at nytemplates.com/blank-new-york-mv51-template.
- VA Form 21-526EZ: This is used to apply for disability compensation and related benefits from the Department of Veterans Affairs. It shares the DD 149's purpose of facilitating access to veteran services.
- DD Form 293: This form is for requesting a review of discharge from the Armed Forces. Similar to the DD 149, it addresses issues related to a service member's discharge status.
- SF 180: The Standard Form 180 is used to request military records. Both this form and the DD 149 are essential for veterans seeking to access their service records for various purposes.
- VA Form 21-534EZ: This form is for survivors of veterans applying for dependency and indemnity compensation. It is similar to the DD 149 in that it supports individuals in navigating veteran-related benefits.
- DD Form 1172: This is the application for a uniformed services identification card. Like the DD 149, it is part of the process to access military benefits and services.
- VA Form 10-10EZ: This application for health benefits from the VA is similar to the DD 149 in its role of helping veterans access necessary services and support.
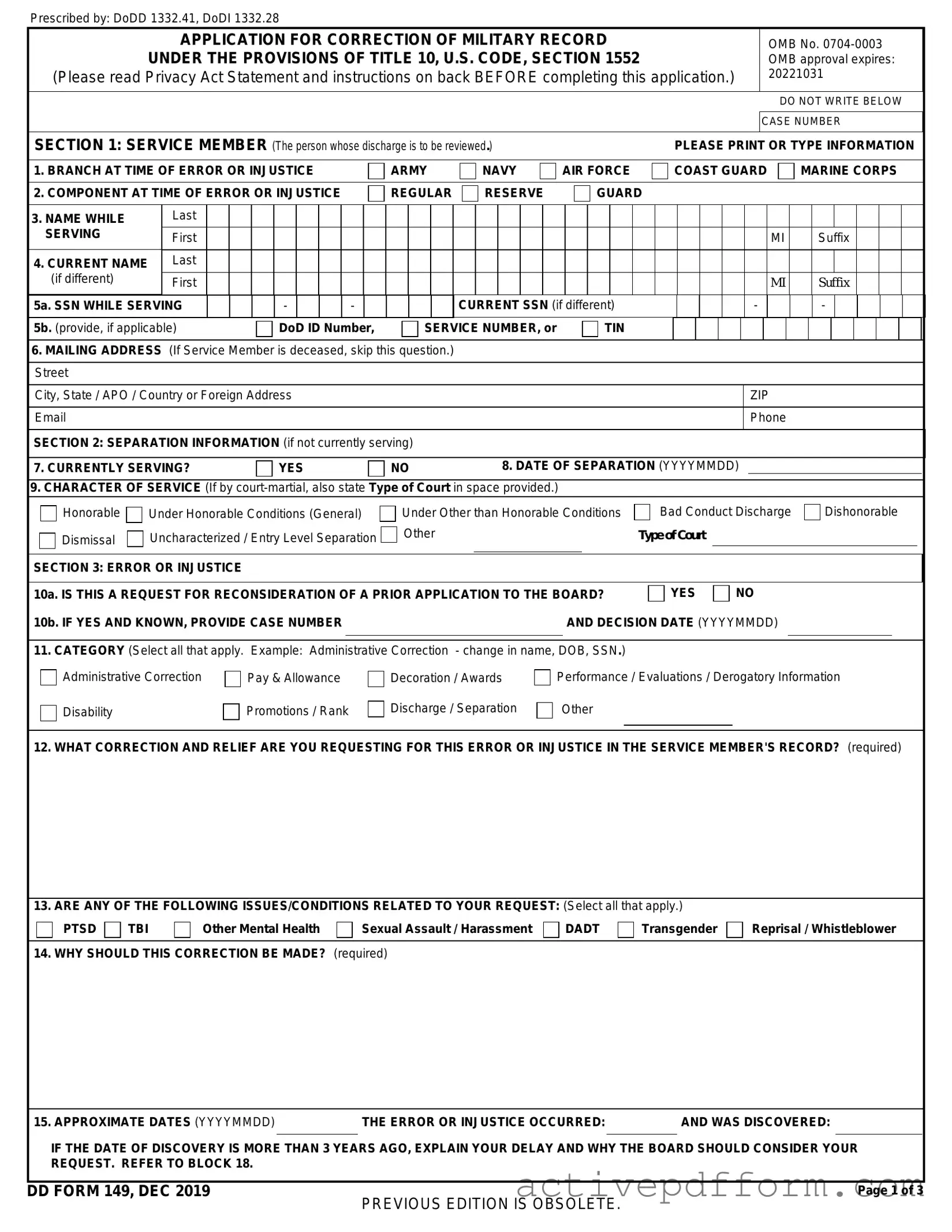
DD 149 Example
Prescribed by: DoDD 1332.41, DoDI 1332.28
APPLICATION FOR CORRECTION OF MILITARY RECORD
UNDER THE PROVISIONS OF TITLE 10, U.S. CODE, SECTION 1552
(Please read Privacy Act Statement and instructions on back BEFORE completing this application.)
OMB No.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DO NOT WRITE BELOW |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASE NUMBER |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 1: SERVICE MEMBER (The person whose discharge is to be reviewed.) |
|
|
|
|
|
|
|
|
|
|
PLEASE PRINT OR TYPE INFORMATION |
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. BRANCH AT TIME OF ERROR OR INJUSTICE |
|
|
|
|
ARMY |
|
|
|
|
NAVY |
|
|
|
AIR FORCE |
|
|
|
COAST GUARD |
|
|
|
MARINE CORPS |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
2. COMPONENT AT TIME OF ERROR OR INJUSTICE |
|
|
|
|
REGULAR |
|
|
|
|
RESERVE |
|
|
|
|
GUARD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. NAME WHILE |
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SERVING |
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI |
|
|
|
Suffix |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. CURRENT NAME |
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(if different) |
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI |
|
|
|
Suffix |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
5a. SSN WHILE SERVING |
|
|
|
- |
|
|
- |
|
|
|
|
|
|
CURRENT SSN (if different) |
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
- |
|
|
|
|
|||||||||||||||||||
5b. (provide, if applicable) |
|
|
|
DoD ID Number, |
|
|
SERVICE NUMBER, or |
|
|
|
|
TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6.MAILING ADDRESS (If Service Member is deceased, skip this question.) Street
City, State / APO / Country or Foreign Address |
ZIP |
|
|
Phone |
|
|
|
SECTION 2: SEPARATION INFORMATION (if not currently serving)
7. CURRENTLY SERVING? |
|
YES |
|
NO |
8. DATE OF SEPARATION (YYYYMMDD) |
||
|
|
|
|
|
|
|
|
9.CHARACTER OF SERVICE (If by
Honorable |
Under Honorable Conditions (General) |
Under Other than Honorable Conditions |
Bad Conduct Discharge |
Dishonorable |
|
|||
Dismissal |
Uncharacterized / Entry Level Separation |
Other |
Type of Court |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 3: ERROR OR INJUSTICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
10a. IS THIS A REQUEST FOR RECONSIDERATION OF A PRIOR APPLICATION TO THE BOARD? |
YES |
NO |
|
|
||||
10b. IF YES AND KNOWN, PROVIDE CASE NUMBER |
|
AND DECISION DATE (YYYYMMDD) |
|
|
||||
11.CATEGORY (Select all that apply. Example: Administrative Correction - change in name, DOB, SSN.)
Administrative Correction |
|
Pay & Allowance |
|
Decoration / Awards |
|
|
Performance / Evaluations / Derogatory Information |
||
|
|
|
|
Discharge / Separation |
|
|
Other |
||
Disability |
|
Promotions / Rank |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
12. WHAT CORRECTION AND RELIEF ARE YOU REQUESTING FOR THIS ERROR OR INJUSTICE IN THE SERVICE MEMBER'S RECORD? (required)
13. ARE ANY OF THE FOLLOWING ISSUES/CONDITIONS RELATED TO YOUR REQUEST: (Select all that apply.)
PTSD  TBI
TBI  Other Mental Health
Other Mental Health  Sexual Assault / Harassment
Sexual Assault / Harassment  DADT
DADT  Transgender
Transgender 
 Reprisal / Whistleblower
Reprisal / Whistleblower
14. WHY SHOULD THIS CORRECTION BE MADE? (required)
15. APPROXIMATE DATES (YYYYMMDD)THE ERROR OR INJUSTICE OCCURRED:AND WAS DISCOVERED:
IF THE DATE OF DISCOVERY IS MORE THAN 3 YEARS AGO, EXPLAIN YOUR DELAY AND WHY THE BOARD SHOULD CONSIDER YOUR REQUEST. REFER TO BLOCK 18.
DD FORM 149, DEC 2019
PREVIOUS EDITION IS OBSOLETE.
Page 1 of 3

 YES. (IN PERSON)
YES. (IN PERSON)
YES. (VIA VIDEO /
TELEPHONE)
NO. CONSIDER MY APPLICATION BASED ON RECORDS & EVIDENCE.
THE BOARD WILL DETERMINE IF WARRANTED.
18.ADDITIONAL REMARKS/CONTINUATION OF INFORMATION (If more space is needed, please submit additional narrative as required.)
SECTION 4: EVIDENCE, RECORDS, AND ADDITIONAL REMARKS
19.IN SUPPORT OF THIS CLAIM, THE FOLLOWING DOCUMENTARY EVIDENCE IS ATTACHED (LIST DOCUMENTS): Example evidence / records: Separation packet, medical documents (e.g. diagnosis, VA rating),
a.
b.
c
d. |
g. |
e. |
h. |
f. |
i. |
|
|
LIST ADDITIONAL SUPPORTING DOCUMENTS (if needed)
IMPORTANT NOTE: If the basis of your request involves the effects of one or more physical, medical, mental, and/or behavioral health condition(s) and if available, please attach copies of any VA rating decisions, relevant medical records, and counseling treatment records.
SECTION 5: CLAIMANT (if other than the Service Member)
20. RELATION TO SERVICE MEMBER
Claimants are normally Service Members seeking to correct their own records. The Service Member or former Service Member is not able to sign the
application because they are |
deceased, |
incapacitated, or |
other |
|
|
|
|
|
||
Please designate appropriate signatory below: |
|
|
|
|
|
|
|
|
||
I am the heir of the Service Member: |
widow(er), |
son, |
daughter, |
parent, |
sibling, |
Other |
|
|||
Please provide Service Member's death certificate and marriage license or heir's birth certificate, as appropriate to prove relationship.
I am the |
conservator, |
guardian, or |
Please provide a notarized power of attorney or court appointment of conservatorship or guardianship to prove status.
I am the |
spouse, |
|
former spouse, or |
|
dependent of the Service Member. |
|
|
|
|
|
|
||||||||||||||||||||||||
Please provide marriage license, divorce decree, or dependent birth certificate, as appropriate to prove relationship |
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. NAME |
|
|
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI |
|
Suffix |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22. MAILING ADDRESS |
|
Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
City, State / APO / Country or Foreign Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ZIP |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 6: REPRESENTATIVE OR COUNSEL (if applicable)
The following representative is authorized to receive and provide communication regarding this application.
23. NAME |
Last |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI |
|
|
Suffix |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. ORGANIZATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
25. MAILING ADDRESS Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
City, State / APO / Country or Foreign Address |
|
|
|
|
|
|
ZIP |
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
SECTION 7: SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
26. I WOULD LIKE TO RECEIVE ALL CORRESPONDENCE & DOCUMENTS ELECTRONICALLY. |
|
|
|
|
|
|
|
|
|
YES |
|
|
|
|
NO |
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
(This may reduce overall processing time.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
CERTIFICATION: I MAKE THE FOREGOING STATEMENTS, AS PART OF THIS CLAIM, WITH FULL KNOWLEDGE OF THE PENALTIES INVOLVED FOR WILLFULLY MAKING A FALSE STATEMENT OR CLAIM. (U.S. Code, Title 18, Section 287 and 1001, provide that an individual shall be fined under this title or imprisoned not more than 5 years, or both.)
|
27a. SIGNATURE |
|
|
27b. DATE SIGNED (YYYYMMDD) |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
16. IS THIS REQUEST RELATED TO ANY |
Operation Freedom Sentinel (OFS) (01/01/2015 - Present) |
Persian Gulf War (08/02/1990 - 11/30/1995) |
||||||
|
Operation Inherent Resolve (OIR) (08/08/2014 - Present) |
Vietnam War (01/01/1961 - 04/30/1975) |
|||||||
|
|
|
OF THESE WARS OR CONTINGENCY |
Operation Enduring Freedom (OEF) (09/11/2001 - |
|
|
|
||
|
|
|
OPERATIONS? |
|
Korean War (06/27/1950 - 07/27/1954) |
||||
|
|
|
|
12/31/2014) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Operation New Dawn (OND) (09/01/2010 - 12/15/2011) |
World War II (12/07/1941 - 09/02/1945) |
|||
|
|
|
Yes (Select all that apply. |
No |
|||||
|
|
|
Operation Iraqi Freedom (OIF) (03/19/2003 - 08/31/2010) |
Other |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 149, DEC 2019 |
|
PREVIOUS EDITION IS OBSOLETE. |
|
Page 2 of 3 |
||||
|
|
|
|
|
|
|
|
||
Prescribed by: DoDD 1332.41, DoDI 1332.28
INSTRUCTIONS FOR COMPLETION OF DD FORM 149
Under Title 10 United States Code Section 1552, current and former members of the Armed Forces, their lawful or legal representatives, spouses and ex- spouses of former members seeking Survivor Benefit Program (SBP) benefits, and civilian employees seeking correction of military records other than those related to civilian employment, who feel that they have suffered an injustice as a result of error or injustice in military records may apply to their respective Boards for Correction of Military (or Naval) Records (BCMR/BCNR) for a correction of their military records. These Boards are the highest level appellate review authority in the military. Therefore, applicants must exhaust all other administrative correction and appeal procedures before applying to the Boards.
This form collects the basic data that the Boards need to process and act on the request. Type or print all entries for all applicable items. If the item is not applicable, enter "NA." If the space provided is insufficient, attach an extra page.
SECTION 3, ITEM 12. State the specific correction of record and all relief desired. If possible, identify exactly what document or information in your record you believe to be erroneous or unjust and indicate what correction you want made to it. For additional errors or injustices, use Section 8.
ITEM 14. To justify correction of a military record, you must explain and show to the satisfaction of the Board that the alleged entry or omission in the record is in error or unjust.
ITEM 15. U.S. Code, Title 10, Section 1552(b), states that no correction may be made unless the request is made within three years after the discovery of the error or injustice, but the Board may excuse failure to file within three years in the interest of justice.
ITEM 16. Indicate whether you attribute the error or injustice to your involvement in a particular war or contingency operation.
ITEM 17. A hearing is not required to ensure the Board's full and impartial consideration of your application. If the Board decides that a hearing is warranted, you, your witnesses, and your counsel may attend at no expense to the government, except that counsel may be provided if the Inspector General has reported reprisal against you.
SECTION 4. You are responsible for obtaining and submitting clear, legible evidence to persuade the Board to grant your request, including any evidence that is not already in your military record. Do not assume a document is in your record. Your evidence should be submitted with this form and may include, for example, military records and orders, witnesses' sworn affidavits, and a brief of arguments supporting your request. List your evidence in item 19 and, if your case involves a medical condition, submit relevant medical records and VA rating decisions as noted in item 20. Do not send irreplaceable original documents because they will not be returned.
SECTION 5. The person whose record will be corrected if relief is granted must sign this form in Section 7. If that person is deceased or incompetent to sign, a lawful claimant, such as a spouse, widow(er), next of kin (child, parent, or sibling), or legal representative, may sign the form. Proof of death, incompetency, or power of attorney must be submitted. Former spouses may apply as claimants for SBP issues
.
SECTION 6. You may want counsel if your case is complex. Some veterans and service organizations furnish counsel without charge. Contact your local post or chapter.
For detailed information on application and Board procedures, see: Army Regulation
|
MAIL COMPLETED APPLICATIONS TO APPROPRIATE ADDRESS BELOW |
|
|
|
|
|
|
ARMY |
NAVY AND MARINE CORPS |
AIR FORCE |
COAST GUARD |
Army Review Boards Agency |
Board for Correction of Naval |
Air Force Board for Correction of |
DHS Office of the General Counsel |
251 18th Street South, Suite 385 |
Records |
Military Records |
Board for Correction of Military |
Arlington, VA |
701 S. Courthouse Rd, Suite 1001 |
3351 Celmers Lane |
Records, Stop 0485 |
http://arba.army.pentagon.mil |
Arlington, VA |
Joint Base Andrews, MD |
2707 Martin Luther King Jr. Ave. S.E. |
|
http://www.secnav.navy.mil/mra/bcnr |
Washington, DC |
|
|
/Pages/default.aspx |
https://www.uscg.mil/Resources/lega |
|
|
|
|
l/BCMR/ |
The public reporting burden for this collection of information is estimated to average 30 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding the burden estimate or burden reduction suggestions to the Department of Defense, Washington Headquarters Services, at
RETURN COMPLETED FORM TO THE APPROPRIATE ADDRESS ON PAGE 3.
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C. 1552, Correction of military records: claims incident thereto; and E.O. 9397 (SSN), as amended.
PRINCIPAL PURPOSE(S): To initiate an application for correction of military record. The form is used by Board members for review of pertinent information in making a determination of relief through correction of a military record. Completed forms are covered by correction of military records SORNs maintained by each of the Services or the Defense Finance and Accounting Service.
ROUTINE USE(S): The DoD Routine Uses can be found in the applicable system of records notices below:
Army
Navy and Marine Corps
Defense Finance and Accounting Service
Official Military Personnel Files:
Army
Marine Corps
DISCLOSURE: Voluntary. However, failure by a claimant to provide the information not annotated as “optional” may result in a denial of your application. A claimant's SSN is used to retrieve these records and links to the member's official military personnel file and pay record.
DD FORM 149, DEC 2019
PREVIOUS EDITION IS OBSOLETE.
Page 3 of 3
Understanding DD 149
What is the DD Form 149?
The DD Form 149, also known as the Application for Correction of Military Records, is a document used by military personnel, veterans, and their families to request changes to military records. This form is essential for correcting errors, updating information, or addressing issues related to discharge status, awards, and other important details. By submitting this form, individuals can ensure that their military records accurately reflect their service and achievements.
Who is eligible to use the DD Form 149?
Eligibility to use the DD Form 149 typically includes active duty members, veterans, and certain family members of deceased service members. If you believe there is an error in your military record or if you need to make a change, you may be eligible to file this application. It's important to note that the form can be submitted by the individual themselves or by someone acting on their behalf, such as a legal representative or a family member.
How do I fill out the DD Form 149?
Filling out the DD Form 149 requires careful attention to detail. Start by providing your personal information, including your name, Social Security number, and service details. Clearly describe the changes you are requesting and provide any supporting documentation that may help your case. This could include copies of discharge papers, awards, or other relevant records. Be sure to sign and date the form before submitting it. A complete and well-documented application increases the likelihood of a favorable outcome.
Where do I submit the DD Form 149?
Once you have completed the DD Form 149, you need to submit it to the appropriate board for correction of military records. This is usually the Board for Correction of Military Records (BCMR) for your specific branch of service. Each branch has its own procedures and mailing addresses, so it’s essential to check the specific requirements for your branch. You can often find this information on the official website of your military branch or by contacting their personnel office directly.
Dos and Don'ts
When filling out the DD 149 form, it’s important to follow certain guidelines to ensure accuracy and completeness. Here are some things you should and shouldn't do:
- Do: Read the instructions carefully before starting the form.
- Do: Use black or blue ink for clarity.
- Do: Provide all requested information completely.
- Do: Double-check for any errors before submission.
- Do: Sign and date the form where required.
- Do: Keep a copy of the completed form for your records.
- Don't: Leave any sections blank unless instructed.
- Don't: Use white-out or correction fluid on the form.
- Don't: Submit the form without verifying your information.
- Don't: Forget to include any required attachments.
- Don't: Use abbreviations that may not be understood.
- Don't: Rush through the process; take your time to ensure accuracy.
Check out Common Templates
I 983 - This form is essential for demonstrating that the training is of a higher degree than mere employment.
Irs Form 14653 - Form 14653 seeks information on the source of funds in foreign financial accounts.
For those looking for clarity in transactions, the "simple Ohio bill of sale documentation" is invaluable. This form not only provides essential details regarding the transfer of ownership but also serves to protect all parties involved. You can explore more about the process at https://formsohio.com/bill-of-sale-online/.
Ucc 308 - Individuals sign the UCC 1-308 to declare their status as sovereign, rejecting certain legal identities.