Free Cna Shower Sheets Template
The CNA Shower Sheets form is a vital tool for ensuring the proper monitoring and documentation of a resident's skin health during bathing. This form facilitates a thorough visual assessment of the skin, allowing Certified Nursing Assistants (CNAs) to identify and record any abnormalities such as bruising, skin tears, rashes, or lesions. Immediate reporting of these issues to the charge nurse is essential for timely intervention and care. The form includes a body chart for CNAs to accurately describe and graph the location of any abnormalities, promoting clear communication among the care team. Additionally, the form prompts the CNA to assess whether the resident requires toenail trimming, which is an important aspect of overall skin care. After the initial assessment, the charge nurse reviews the findings and documents their assessment, ensuring that any necessary interventions are noted and that the information is forwarded to the Director of Nursing (DON) when needed. This systematic approach not only enhances the quality of care provided to residents but also helps maintain compliance with health regulations.
Document Specifics
| Fact Name | Description |
|---|---|
| Purpose | The CNA Shower Sheets form is used for documenting skin assessments during resident showers. |
| Skin Monitoring | It requires a visual assessment of the resident's skin, noting any abnormalities immediately. |
| Report Protocol | Any skin abnormalities must be reported to the charge nurse right away. |
| Body Chart | The form includes a body chart for documenting the location and description of skin issues. |
| Common Abnormalities | It lists various skin conditions such as bruising, rashes, and lesions to assess. |
| Toenail Care | The form includes a section to indicate whether the resident needs toenail trimming. |
| Signatures Required | Both the CNA and the charge nurse must sign the form to confirm the assessment. |
| Governing Law | This form is governed by Missouri state regulations for healthcare documentation. |
Similar forms
- Skin Assessment Form: Similar to the CNA Shower Sheets, this document also focuses on evaluating a resident's skin condition. It includes sections for noting abnormalities and requires reporting to a supervising nurse.
- Eviction Process Forms: Similar to patient assessment documents, these forms outline the necessary steps for landlords to initiate the eviction process, ensuring compliance with local laws. For more details, refer to the Arizona PDF Forms.
- Incident Report: This form is used to document any unexpected events or injuries that occur within a care setting. Like the CNA Shower Sheets, it emphasizes the importance of timely reporting and thorough documentation.
- Daily Care Log: This document records daily activities and observations related to resident care. It shares a similar purpose of monitoring and reporting changes in a resident’s condition, ensuring continuity of care.
- Patient Assessment Tool: This tool is used to evaluate various aspects of a resident's health, including skin integrity. It parallels the CNA Shower Sheets in its comprehensive approach to assessing and documenting health concerns.
- Wound Assessment Form: This form specifically addresses the evaluation of wounds and skin integrity. It aligns with the CNA Shower Sheets by providing detailed criteria for identifying and documenting skin issues.
- Medication Administration Record (MAR): The MAR tracks medications given to residents. While focused on medication, it shares the need for accuracy and thorough documentation, similar to the CNA Shower Sheets.
- Care Plan: This document outlines the individualized care strategies for each resident. It is similar in that it requires ongoing assessments and adjustments based on the resident's changing needs, much like the skin monitoring aspect of the CNA Shower Sheets.
Cna Shower Sheets Example
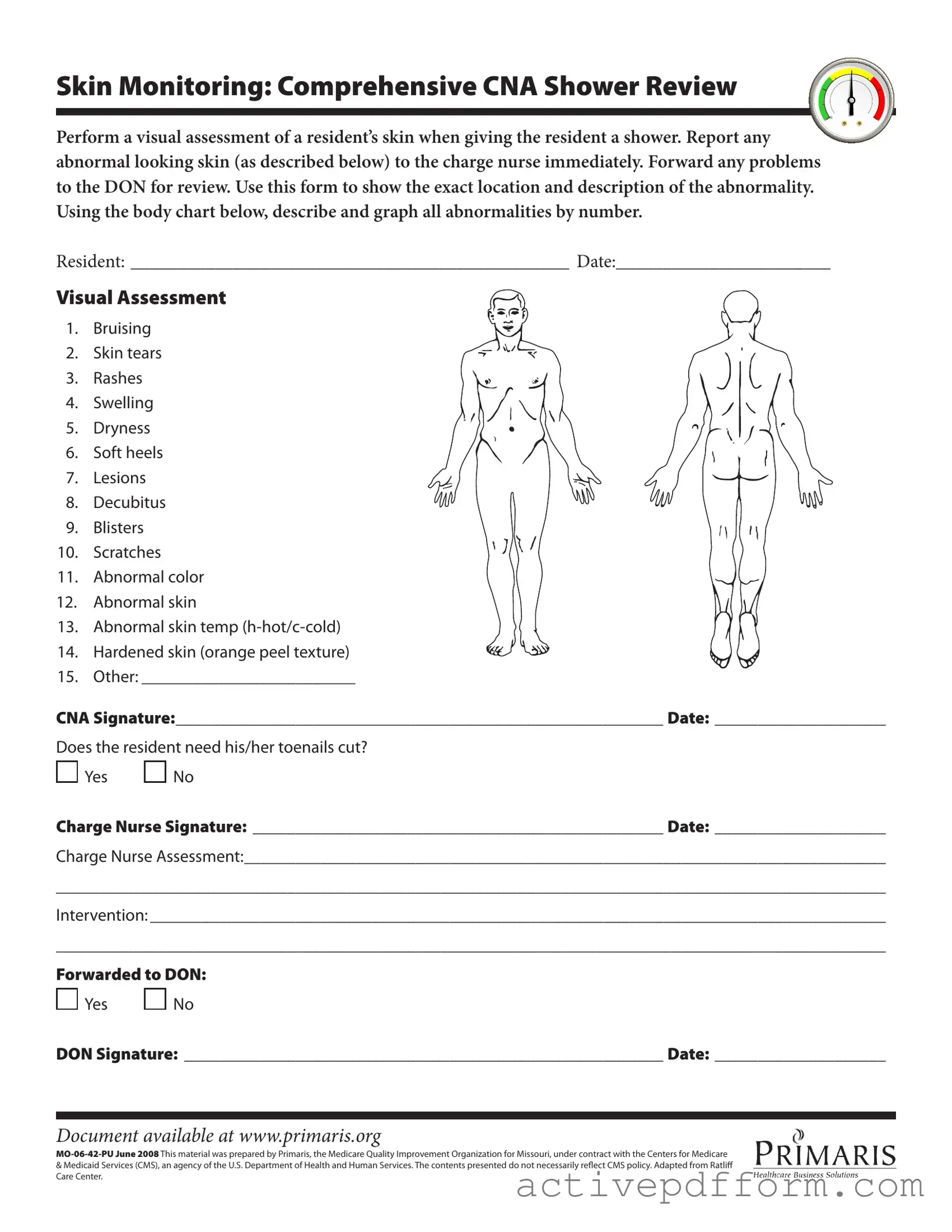
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Understanding Cna Shower Sheets
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to facilitate the visual assessment of a resident's skin during showering. It allows Certified Nursing Assistants (CNAs) to document any abnormalities they observe, ensuring that any issues are reported promptly to the charge nurse and subsequently reviewed by the Director of Nursing (DON).
What types of skin abnormalities should be reported?
CNAs should look for various skin abnormalities during their assessments. These include bruising, skin tears, rashes, swelling, dryness, soft heels, lesions, decubitus ulcers, blisters, scratches, abnormal color, abnormal skin texture, and abnormal skin temperature. Any of these findings should be documented on the form.
How should abnormalities be documented on the form?
Abnormalities should be documented by describing their exact location and providing a brief description. CNAs should use the body chart included in the form to graphically represent all abnormalities by numbering them. This visual representation aids in accurate reporting and follow-up.
What should be done if an abnormality is found?
If a CNA identifies any abnormal skin conditions, they must report these findings to the charge nurse immediately. The charge nurse will then assess the situation and determine the appropriate intervention. Any significant issues will be forwarded to the DON for further review.
Is there a section for documenting toenail care?
Yes, the form includes a section where CNAs can indicate whether the resident needs their toenails cut. This is an important aspect of personal care that can impact a resident's overall comfort and health.
What is the role of the charge nurse in this process?
The charge nurse is responsible for reviewing the CNA's findings and conducting their own assessment. They will document their observations on the form and decide on any necessary interventions. Their signature on the form indicates that they have completed this assessment.
What happens after the charge nurse assesses the resident?
After the charge nurse completes their assessment, they may implement interventions based on their findings. If necessary, they will forward the information to the DON for further evaluation. This ensures that all relevant parties are informed and can take appropriate action.
What does it mean if the form is forwarded to the DON?
If the form is marked as forwarded to the DON, it indicates that the charge nurse has identified issues that require additional review or intervention. This step is crucial for ensuring that serious conditions are monitored and addressed in a timely manner.
Where can I access the CNA Shower Sheets form?
The CNA Shower Sheets form is available online at www.primaris.org. It is important to use the most current version to ensure compliance with guidelines set forth by health authorities.
What should I do if I have questions about the form?
If you have questions about the CNA Shower Sheets form or its use, it is advisable to consult with your supervisor or the charge nurse. They can provide guidance and clarification on how to properly complete the form and address any specific concerns.
Dos and Don'ts
When filling out the CNA Shower Sheets form, attention to detail is crucial. This form plays a vital role in monitoring residents' skin health and ensuring proper care. Here’s a list of things you should and shouldn’t do to make the process smoother and more effective.
- Do perform a thorough visual assessment of the resident’s skin during the shower.
- Do report any abnormalities to the charge nurse immediately.
- Do use the body chart to accurately describe and graph any abnormalities.
- Do ensure that all sections of the form are filled out completely.
- Don't ignore any signs of skin issues; even minor concerns should be documented.
- Don't forget to sign and date the form after completing it.
- Don't leave any questions unanswered; clarity is essential for effective communication.
Completing this form accurately not only helps in providing quality care but also ensures that residents' health is prioritized. Take the time to do it right, and always keep the lines of communication open with your team.
Check out Common Templates
Planned Parenthood Pregnancy Verification Letter - The Planned Parenthood Proof form is designed for patients in Southeastern Virginia to maintain confidentiality while seeking medical services.
In order to successfully complete the application process for the New York DTF-84 form, businesses can turn to various resources that provide guidance and templates, such as nytemplates.com/blank-new-york-dtf-84-template, which can be instrumental in ensuring all paperwork is filled out accurately and meets the requirements set by Empire State Development.
Yes/no/maybe List - Interest in experiencing light beatings with hands, focusing on trust and communication.
Hvac Job Application - Choose specific industry skills that highlight your expertise and competencies.