Free Annual Physical Examination Template
The Annual Physical Examination form serves as a crucial tool in promoting health and well-being for individuals of all ages. This comprehensive document collects essential information before a medical appointment, ensuring that healthcare providers have a clear understanding of a patient’s medical history, current medications, and any significant health conditions. The first part of the form requires personal details such as name, date of birth, and social security number, as well as a summary of diagnoses and chronic health issues. It also includes a section for current medications, allergies, and immunization records, which are vital for assessing a patient's overall health status. Additionally, the form addresses tuberculosis screening, communicable diseases, and various medical tests, such as GYN exams and blood work, tailored to different age groups and genders. The second part focuses on the general physical examination, where vital signs and evaluations of various body systems are documented. This thorough approach not only facilitates accurate diagnoses but also fosters a proactive dialogue between patients and healthcare providers about ongoing health maintenance and necessary lifestyle adjustments. By completing this form diligently, individuals help ensure a more effective and personalized healthcare experience.
Document Specifics
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Annual Physical Examination Form is designed to collect comprehensive health information from patients before their medical appointments. |
| Information Required | Patients must provide personal details such as name, date of birth, address, and Social Security Number to ensure accurate medical records. |
| Medical History | Patients are asked to disclose diagnoses and significant health conditions, along with a list of current medications and allergies. |
| Immunization Records | The form includes sections for documenting immunizations, such as Tetanus, Hepatitis B, and Influenza, along with their administration dates. |
| Screening Tests | Patients must report results from various screenings, including tuberculosis, GYN exams, and prostate exams, as appropriate for their age and gender. |
| Physical Examination Details | Key metrics such as blood pressure, pulse, and weight are recorded to assess the patient's overall health during the examination. |
| Evaluation of Systems | The form includes a checklist for evaluating different body systems, allowing healthcare providers to identify any abnormalities. |
| Recommendations for Health | Healthcare providers may include recommendations for health maintenance, such as dietary advice and exercise plans, based on the examination findings. |
| Legal Requirements | In many states, specific laws govern the collection and storage of medical information, ensuring patient confidentiality and informed consent. |
| Importance of Completion | Completing all sections of the form is crucial to avoid return visits and ensure that healthcare providers have all necessary information for effective care. |
Similar forms
- Patient Intake Form: Similar to the Annual Physical Examination form, the Patient Intake Form gathers essential information about the patient’s medical history, current medications, and personal details before a medical appointment. Both documents aim to ensure that healthcare providers have a comprehensive understanding of the patient's background to deliver appropriate care.
- Health History Questionnaire: This document collects detailed information about past illnesses, surgeries, and family medical history. Like the Annual Physical Examination form, it emphasizes the importance of understanding a patient's health trajectory to inform future medical decisions.
- Medication Reconciliation Form: This form tracks current medications and dosages, similar to the section in the Annual Physical Examination form. It helps prevent medication errors and ensures that healthcare providers are aware of all substances the patient is taking.
- Immunization Record: Both documents include sections for immunizations received. The Annual Physical Examination form details specific vaccines and dates, while an Immunization Record serves as a comprehensive log of all vaccinations a patient has received throughout their life.
- Consent for Treatment Form: This form ensures that patients understand and agree to the treatments they will receive. Like the Annual Physical Examination form, it requires a signature and serves as an important legal document in the patient-care provider relationship.
- Referral Form: When a patient needs to see a specialist, a Referral Form is often completed. This document, like the recommendations section of the Annual Physical Examination form, outlines the reason for the referral and any pertinent medical history that the specialist should consider.
- Lab Test Requisition Form: This form requests specific laboratory tests to be performed, similar to the section on medical tests in the Annual Physical Examination form. Both documents ensure that necessary evaluations are conducted to assess the patient’s health status.
- Physical Therapy Evaluation Form: Used when a patient is referred for physical therapy, this form gathers information about the patient's physical condition and goals. Like the Annual Physical Examination form, it assesses the patient’s current health and outlines a plan for treatment.
- Power of Attorney Form: This form is crucial as it allows individuals to designate someone they trust to make decisions on their behalf in legal or financial matters. It ensures that their preferences are respected, especially in times of incapacity. To fill out the form, please visit Arizona PDF Forms.
- Follow-Up Appointment Form: This document is used to schedule and confirm follow-up visits after an initial examination. It is similar to the Annual Physical Examination form in that it emphasizes continuity of care and the importance of regular health monitoring.
Annual Physical Examination Example

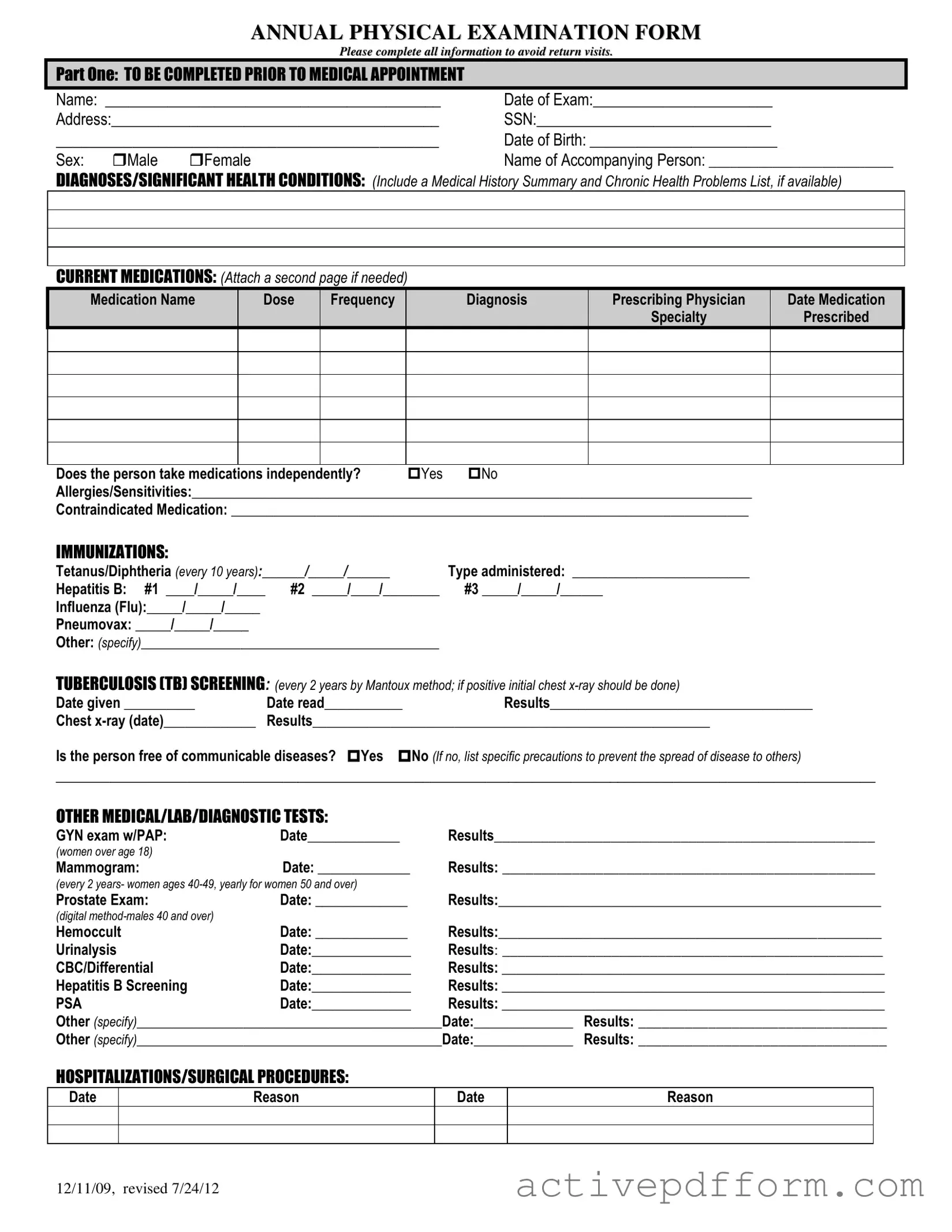
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12
PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
Understanding Annual Physical Examination
What is the purpose of the Annual Physical Examination form?
The Annual Physical Examination form serves as a comprehensive tool for healthcare providers to gather essential information about a patient’s health before their medical appointment. It includes sections for personal details, medical history, current medications, immunizations, and results from various diagnostic tests. By completing this form, patients help ensure that their healthcare providers have the necessary information to deliver effective care and make informed decisions regarding their health.
What information should I include in the medical history section?
In the medical history section, it is important to include any significant health conditions or diagnoses that you may have. This can include chronic illnesses, past surgeries, and any ongoing treatments. If available, a summary of your medical history and a list of chronic health problems can provide valuable context for your healthcare provider. This information helps them understand your health background and tailor their examination and recommendations accordingly.
How do I report my current medications on the form?
When reporting your current medications, list each medication name along with its dosage, frequency, the diagnosis it is prescribed for, and the name of the prescribing physician. If you take multiple medications, feel free to attach a separate page to ensure that all information is captured clearly. Additionally, indicate whether you take these medications independently or require assistance. This thorough reporting allows healthcare providers to monitor potential interactions and adjust treatments as necessary.
What should I do if I have allergies or sensitivities?
If you have any allergies or sensitivities, it is crucial to list them on the form. This includes allergies to medications, food, or environmental factors. Additionally, if there are any medications that are contraindicated for you, those should be noted as well. Providing this information helps ensure your safety during medical procedures and when prescribing medications, allowing healthcare providers to make informed choices that minimize the risk of adverse reactions.
Dos and Don'ts
Things to Do:
- Read the entire form carefully before filling it out.
- Provide accurate personal information, including your name and date of birth.
- List all current medications, including dosage and frequency.
- Disclose any allergies or sensitivities clearly.
- Complete all sections, even if some information seems unnecessary.
- Sign and date the form at the end to confirm the accuracy of your information.
- Attach any additional pages if you need more space for medications or medical history.
- Double-check for any missed questions or incomplete sections before submission.
- Bring the completed form to your appointment to avoid delays.
Things to Avoid:
- Do not leave any sections blank unless instructed.
- Avoid using abbreviations that may confuse the medical staff.
- Do not provide outdated or incorrect medical history.
- Refrain from omitting important health conditions or previous surgeries.
- Do not guess on answers; if unsure, indicate that you do not know.
- Do not forget to include the name of the prescribing physician for medications.
- Avoid using vague language; be specific in your descriptions.
- Do not submit the form without reviewing it for errors.
- Do not wait until the last minute to fill out the form; complete it well in advance of your appointment.
Check out Common Templates
T-47 Description of Property - The affidavit must be submitted to the title company handling the transaction.
The proper completion of the New York MV51 form is vital for ensuring a seamless transfer of ownership for older vehicles, including those from 1972 or earlier, and non-titled vehicles. For those seeking more information about this essential certification document, you can visit https://nytemplates.com/blank-new-york-mv51-template/ to access templates that can help facilitate the process of private vehicle sales and ensure legal compliance.
How Do You File a Mechanics Lien - The form helps to establish a legal interest in the property for unpaid contractors.